
Adipotide peptide is an experimental prohibitin-targeting peptidomimetic also known as FTPP or Prohibitin-TP01, studied because it was designed to bind targets in the vasculature of white adipose tissue and trigger apoptosis in that tissue environment 1. This educational guide reviews its proposed mechanism, obesity and metabolic research, early human trial context, published study dosing, side effects, safety limits, and regulatory status. It does not provide personal dosing, injection, purchasing, or treatment instructions.
- Adipotide is experimental. NCI describes prohibitin-targeting peptide 1 as a chimeric 25-mer peptide with a fat-targeting motif, proapoptotic motif repeats, and a GG linker [1].
- Its research focus is unusual. Rather than acting mainly through appetite hormones, Adipotide was designed to target blood vessels supplying white adipose tissue, a concept supported mainly by preclinical models [1]2.
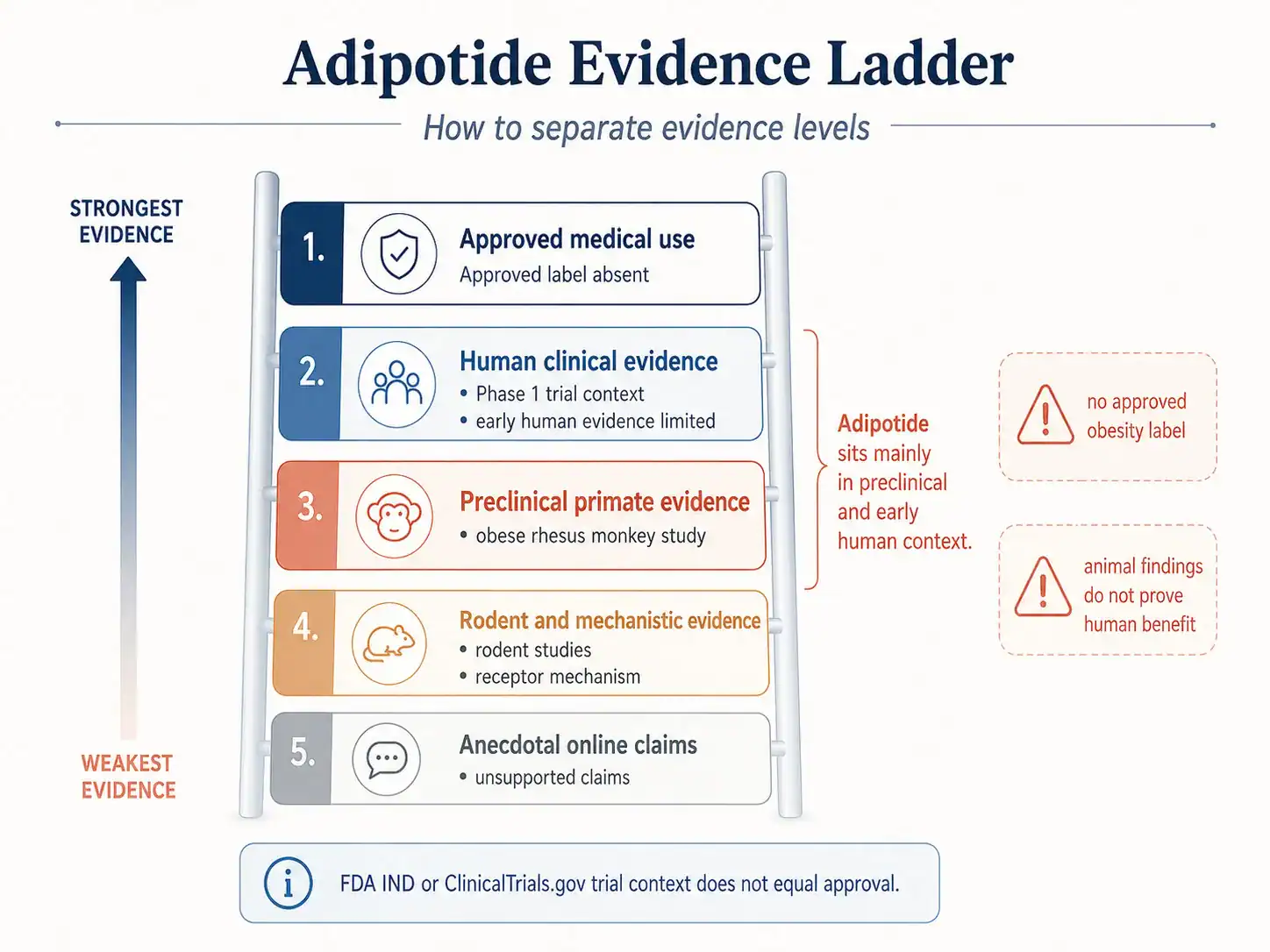
- The strongest obesity-related findings are preclinical. Obese rhesus monkey and rodent studies reported reductions in body weight, white fat measures, and metabolic markers, but these findings do not establish an approved human obesity treatment [2]3.
- Human evidence is early and limited. A registered Phase 1 study evaluated Prohibitin-TP01 in patients with advanced prostate cancer and obesity to identify a maximum tolerated dose, not to prove general obesity efficacy 8.
- Safety questions are central. The primate study reported predictable and reversible renal proximal tubule changes at experimentally determined doses, making kidney-related monitoring a key research concern [2].
- Dosage information is study context only. Published animal dosing and the Phase 1 design should not be converted into personal dosing advice [2]10.
- Regulatory status matters. Adipotide is discussed in investigational and clinical-trial context, not as an FDA-approved anti-obesity medication with approved labeling [8]911.
Related dosage pages: For vial-specific concentration, reconstitution, and measurement examples, see Adipotide (10 mg Vial) Dosage Protocol. Each linked protocol remains a separate reference because vial strength changes concentration and syringe-unit calculations.
Fast Answer
Adipotide peptide is an experimental prohibitin-targeting peptidomimetic, also called FTPP or Prohibitin-TP01, designed to target blood vessels in white adipose tissue and trigger apoptosis in selected adipose-associated endothelium [1]. It is searched for obesity and metabolic research because animal studies reported reduced body weight, white fat, and insulin-resistance markers, but human evidence remains limited to Phase 1 trial context and there is no approved obesity dosing label [2][8]. Safety questions, especially kidney and vascular effects, remain central [2].
What Is the Adipotide Peptide?
Adipotide is a synthetic targeted peptide research compound built around the idea that white fat tissue depends on its microvasculature for growth, oxygen, nutrient exchange, and metabolic signaling [1]5. Its public scientific record is strongest in animal and mechanistic research, not in approved human care [2][8].
Obesity is commonly defined in adults as a body mass index of 30.0 or higher, but BMI alone does not capture all aspects of metabolic risk, fat distribution, or individual health status 12. That matters because Adipotide research often uses outcomes such as body weight, BMI, abdominal circumference, glucose tolerance, insulin resistance, and white adipose tissue mass [2].
Adipotide, FTPP, and Prohibitin-Targeting Peptide 1
Adipotide is also referred to as FTPP, fat-targeted proapoptotic peptide, and Prohibitin-TP01 in scientific and regulatory-adjacent sources [1][9]. NCI describes prohibitin-targeting peptide 1 as a 25-mer peptide that targets prohibitin and includes the fat-targeting motif CKGGRAKDC, two repeats of the proapoptotic KLAKLAK motif, and a GG linker [1].
This naming can be confusing for readers because “Adipotide,” “FTPP,” and “Prohibitin-TP01” may appear in different contexts. In this article, Adipotide refers to the same investigational peptide concept unless a study uses a specific research name [1][8].
Peptide Classification, Structure, and White Fat Targeting
Adipotide is often described as a peptidomimetic rather than a conventional endogenous hormone peptide because it combines a targeting motif with a cell-death-inducing motif [1][2]. The primate study described the ligand-directed peptidomimetic CKGGRAKDC-GG-D(KLAKLAK)2, henceforth termed adipotide, in obese Old World monkeys [2].
The “white fat targeting” concept is based on binding in white adipose tissue vasculature, especially endothelial structures associated with white fat tissue [1][3]. That is different from medications that primarily change appetite, nutrient absorption, incretin signaling, or energy expenditure 1516.
Why Is Adipotide Discussed in Obesity Research?
Adipotide is discussed in obesity research because animal studies tested whether targeting the blood vessels supplying white adipose tissue could reduce adipose tissue mass [2][3]. The 2011 Science Translational Medicine study reported that Adipotide treatment induced targeted apoptosis within blood vessels of white adipose tissue and was associated with weight loss and improved insulin-resistance markers in obese monkeys [2].
The reason this drew attention is that adipose tissue expansion is closely linked to blood vessel growth and vascular support [5]. Still, a plausible vascular mechanism does not make Adipotide an approved anti-obesity medication or prove clinical benefit in humans [8][11].
How Does Adipotide Peptide Work?
Adipotide is proposed to work by homing to molecular targets on blood vessels associated with white adipose tissue and delivering a proapoptotic signal [1][2]. In plain language, the research idea is to damage selected blood vessel cells that supply white fat, which may then reduce support for nearby fat cells in animal models [1][3].
Which Blood Vessels Supplying White Adipose Tissue Are Targeted?
The proposed target is the vasculature of white adipose tissue rather than all blood vessels in the body [1][2]. NCI states that the peptide binds specifically to prohibitin in white adipose vasculature and that receptor-mediated internalization triggers apoptosis [1].
The selectivity question is still important. Prohibitin is a multifunctional protein involved in cell survival, growth, and other biological processes, and later work has examined interactions involving prohibitin and annexin A2 in white adipose tissue biology [1]4.
Why Does Vascular Targeting Differ From Appetite Suppression?
Adipotide’s proposed mechanism differs from appetite-suppressing or incretin-based obesity medications because it is aimed at adipose vasculature rather than central hunger pathways or GLP-1/GIP receptors [1][15][16]. FDA-approved medications such as tirzepatide and semaglutide have approved indications, labeled dosing, contraindications, warnings, and human trial data in specific populations, while Adipotide does not have an FDA-approved obesity label [15][16]17.
That distinction matters for searchers comparing “fat loss peptides.” A compound can show striking animal findings and still remain far from an approved therapy if human efficacy, safety, dosing, manufacturing, and labeling have not been established [11].
Mechanism of Action: Receptor Targeting and Apoptosis
The proposed mechanism of action has two linked parts: a homing sequence that binds a vascular target and a proapoptotic sequence that can induce cell death after internalization [1][2]. The scientific hypothesis is biologically plausible, but mechanism alone is not enough to establish human clinical outcomes [11].
What Is the Proposed Receptor System Targeted by Adipotide?
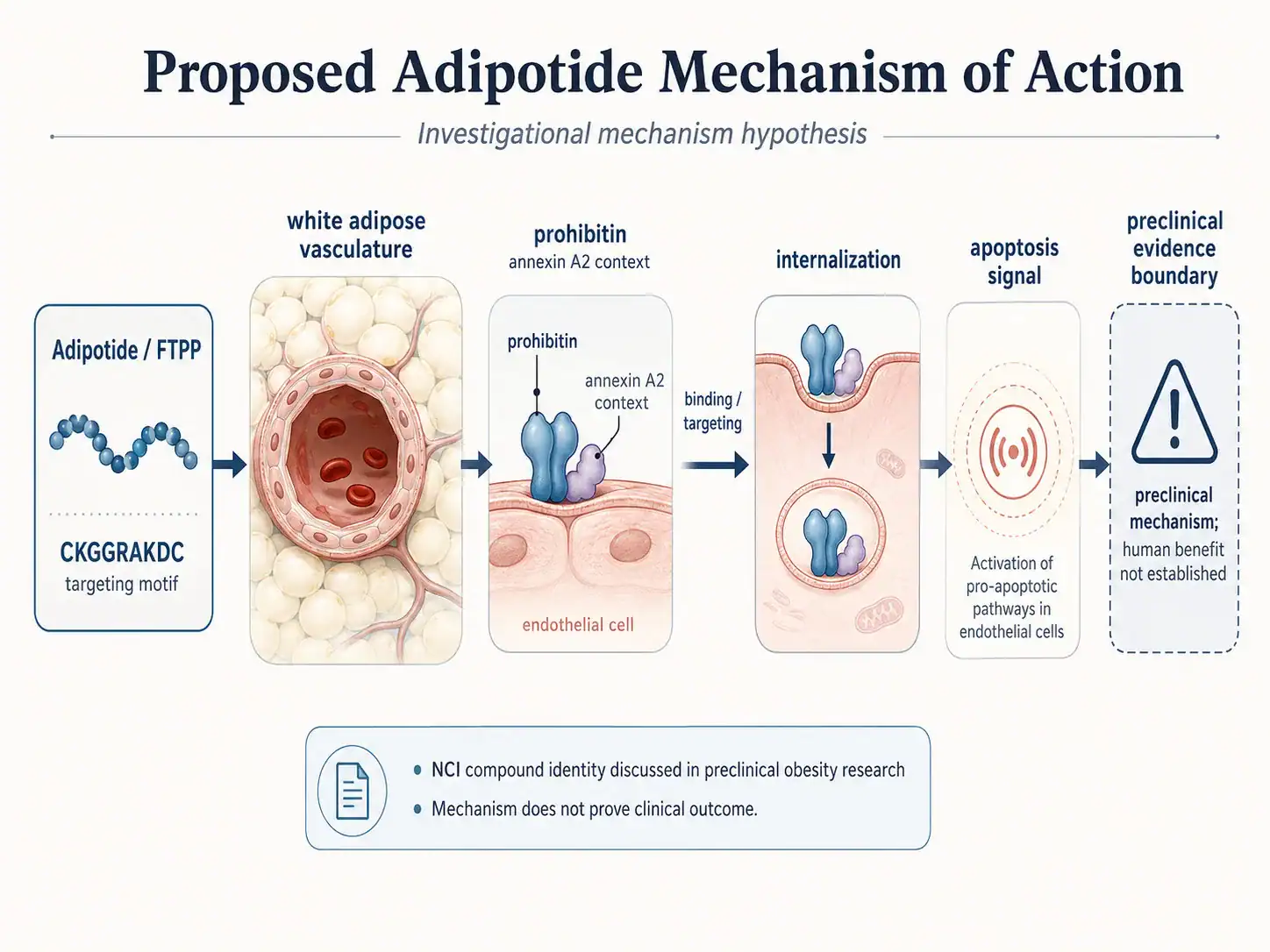
NCI identifies prohibitin as the target of prohibitin-targeting peptide 1 in white adipose vasculature [1]. Later mechanistic work reported that prohibitin and annexin A2 interact on the surface of vascular endothelial cells in white adipose tissue and can participate in fatty acid transport with CD36 in adipose tissue [4].
This receptor-system discussion helps explain why Adipotide is described as a targeted peptide. It does not prove that the same receptor activity will produce safe, durable, or clinically meaningful fat loss in people [8][11].
How Might a Homing Peptide Deliver a Proapoptotic Signal?
The homing peptide motif is intended to guide the compound toward adipose-associated vasculature, while the KLAKLAK-based motif is intended to provide the proapoptotic payload [1][3]. In mouse research, targeting a proapoptotic peptide to prohibitin in the adipose vasculature caused ablation of white fat and rapid obesity reversal in that model [3].
The central idea is targeted cellular injury, not simple “fat burning.” That is why safety questions are more complex than with nutrients, supplements, or standard lifestyle interventions [1][2].
Why Does Mechanism Not Prove Human Fat Loss Outcomes?
Mechanism studies can show how a compound might work, but they cannot replace controlled human studies that measure efficacy, adverse events, dose-response, durability, and patient selection [11]. FDA explains that clinical research progresses through phases and that Phase 3 studies are generally designed to demonstrate whether a product offers treatment benefit in a defined population [11].
For Adipotide, the evidence base remains heavily weighted toward preclinical research and Phase 1 context [2][8]. That makes strong claims about human fat loss, glucose control, or obesity care inappropriate.
What Is Adipotide Peptide Used For or Studied For?
Adipotide has been studied mainly for obesity-related adipose tissue reduction in animals and in a limited human oncology-adjacent context involving advanced prostate cancer and obesity [2][8][10]. It is not an approved medication for obesity, metabolic syndrome, diabetes, or prostate cancer [8][11][17].
Which Obesity, Body Weight, and White Fat Outcomes Are Studied?
The primate study measured body weight, body mass index, abdominal circumference, MRI findings, dual-energy X-ray absorptiometry, and metabolic markers in obese rhesus monkeys [2]. In a fixed-dose study, treated obese monkeys received 0.43 mg/kg subcutaneously daily for 28 days followed by a recovery period, and the study reported average decreases in body weight, BMI, and abdominal circumference [2].
These outcomes are meaningful in animal research, but they are not the same as approved clinical endpoints in humans. Human obesity treatment decisions require validated efficacy and safety data in the intended population [11][15][16].
What Metabolic, Insulin Resistance, and Glucose Measures Matter?
Adipotide research has examined insulin resistance, insulin response, glucose tolerance, and related metabolic markers [2]7. A Diabetes study reported rapid and weight-independent improvement of glucose tolerance in obese mice after a peptide designed to induce apoptosis in white adipose tissue endothelium, but this remains preclinical evidence [7].
These findings support further mechanistic interest. They do not establish Adipotide as a treatment for insulin resistance, prediabetes, or type 2 diabetes in humans [7][11].
Potential Benefits of Adipotide Peptide
Potential benefits must be separated by evidence level. The strongest reported benefits come from animal studies, while human therapeutic benefits remain unproven and regulatory approval has not been established [2][8][11].
What Does Research Suggest About Fat Tissue Reduction?
Preclinical studies suggest that targeting white adipose tissue vasculature can reduce white fat tissue in animal models [2][3]. In obese monkeys, imaging with MRI and dual-energy X-ray absorptiometry confirmed a reduction in white adipose tissue after Adipotide treatment [2].
This is a preclinical benefit signal. It should not be rewritten as “Adipotide causes fat loss in humans” because the available public evidence does not support that clinical claim [8][11].
Evidence for Weight Loss and Improved Insulin Resistance in Obese Models
The 2011 primate study reported rapid weight loss and improved insulin resistance in obese monkeys, with body composition changes measured by imaging [2]. Earlier mouse research reported that targeting a proapoptotic peptide to prohibitin in adipose vasculature caused white fat ablation and obesity reversal in that model [3].
This phrase from the literature—“weight loss and improved insulin resistance in obese monkeys”—is accurate only when tied to the animal model [2]. It should not be used as a direct claim about people.
What Is Known About Food Intake and Body Weight?
Animal work has examined whether changes in food intake contribute to body weight outcomes after vascular-targeted adipose interventions [2]6. A 2010 Diabetes study reported that a peptide designed to elicit apoptosis in adipose tissue endothelium reduced food intake and body weight in high-fat-diet animal models [6].
The food-intake interpretation has also been debated. A published comment argued that the monkey findings might reflect direct effects on food consumption, and the original authors published a response defending their interpretation 1819.
What Human Evidence Exists for Adipotide?
Human evidence is limited. The key public human record is a first-in-man Phase 1 study of Prohibitin-TP01 in patients with advanced prostate cancer and obesity, with the stated goal of finding the highest tolerable dose in that population [8].
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| Compound identity | NCI describes Prohibitin-TP01 as a chimeric 25-mer peptide that targets prohibitin [1]. | Source/database identity | Supports nomenclature and proposed target; does not prove clinical benefit. |
| Obese primate research | Obese rhesus monkeys treated with Adipotide had reduced body weight, BMI, abdominal circumference, and white adipose tissue measures [2]. | Preclinical | Supports animal efficacy signals; cannot establish approved human obesity treatment. |
| Rodent adipose-vascular research | Mouse studies tested targeted ablation of adipose tissue and adipose endothelium effects [3][6][7]. | Preclinical | Supports mechanism and translational hypotheses; animal biology may not predict human outcomes. |
| Human Phase 1 context | ClinicalTrials.gov lists a first-in-man Phase 1 study in advanced prostate cancer and obesity [8]. | Early human | Supports investigational exposure context; does not establish broad efficacy. |
| Approved medical use | FDA drug databases identify official sources for approved drug products, while Adipotide’s public record is investigational [8][11][17]. | No approved use identified | Means no approved label, indication, or dosing instructions are available for patient care. |
| Online fat-loss claims | FDA has warned about unapproved weight-loss products falsely marketed as research-use products in related peptide/drug spaces 14. | Unsupported for Adipotide | Online claims should not be treated as evidence of safety, quality, or efficacy. |
Why Does First-in-Human Phase 1 Context Matter?
Phase 1 context matters because early clinical studies are commonly designed to evaluate safety, tolerability, pharmacokinetics, and dose escalation rather than prove broad therapeutic effectiveness [10][11]. The Adipotide Phase 1 announcement stated that the trial would evaluate a single 28-day cycle, identify a maximum tolerated dose, assess pharmacokinetics, measure weight change, and monitor disease progression [10].
That design does not support self-directed obesity use. It supports the narrower conclusion that Adipotide entered limited human testing under investigational conditions [8][10].
How Do Advanced Prostate Cancer and Obesity Shape Interpretation?
The registered trial population was not a general obesity population; it involved patients with advanced prostate cancer and obesity [8][10]. Arrowhead’s announcement stated that MD Anderson investigators were interested in whether reducing white fat could affect prostate cancer growth, which makes the study oncology-adjacent rather than a standard obesity-drug efficacy trial [10].
This context limits interpretation. Results from patients with advanced cancer, if available, would not automatically apply to otherwise healthy people seeking weight loss [8][10][11].
What Does Missing Published Results Mean for Evidence Quality?
A registered Phase 1 trial and company announcements do not provide the same level of evidence as published, peer-reviewed, controlled human efficacy trials [8][10][11]. For readers, the practical meaning is that Adipotide’s human evidence should be treated as early and incomplete.
The strongest conclusions remain: Adipotide has a defined experimental mechanism, meaningful animal data, and important safety questions, but no approved human obesity indication [1][2][8][11].
What Does Preclinical Evidence Suggest About Adipotide?
Preclinical evidence suggests that adipose-vascular targeting can influence body weight, white fat tissue, insulin resistance, and glucose measures in animal models [2][3][6][7]. This is the main reason for scientific interest in the compound.
What Obese Rhesus Monkey Findings Matter?
The obese rhesus monkey study matters because primate models are often viewed as more translational than rodent models for some metabolic questions [2]. The study reported targeted apoptosis within blood vessels of white adipose tissue, reduced white adipose tissue by imaging, and improved insulin resistance measures [2].
The same study also reported renal proximal tubule changes in monkeys at experimentally determined doses, described as predictable and reversible [2]. That safety signal is part of the evidence, not a footnote.
How Rodent Models Inform White Adipose Tissue Vasculature
Rodent studies helped establish the idea that adipose tissue mass can be regulated through blood vessels and that targeting adipose vasculature can affect fat tissue biology [3][5][6]. In the 2004 Nature Medicine paper, targeting a proapoptotic peptide to prohibitin in adipose vasculature caused ablation of white fat in mice [3].
Rodent evidence is useful for mechanism discovery. It is weaker than human evidence for predicting real-world safety, efficacy, and dose-response in patients [11].
Which Endpoints Track Body Fat, BMI, Glucose Tolerance, and Insulin Sensitivity?
Useful endpoints in Adipotide research include body weight, body mass index, abdominal circumference, white adipose tissue volume, glucose tolerance, insulin response, serum creatinine, and renal histology [2][7]. These endpoints help connect body composition, metabolic function, and toxicity in animal models [2][7].
The most responsible interpretation is endpoint-specific. A reduction in white adipose tissue in a monkey study is not the same as a durable improvement in human obesity outcomes, cardiovascular risk, or diabetes complications [2][11].
Evidence Limitations and Unsupported Online Claims
Adipotide is often discussed online with stronger language than the evidence supports. Claims about targeted fat loss, belly-fat reduction, or obesity treatment should be filtered through evidence level, safety data, and regulatory status [2][8][14].
Why Anecdotal Fat Loss Claims Need Caution
Anecdotal reports cannot establish product identity, purity, dose, adverse-event rates, or causality. FDA has warned that products falsely labeled “for research purposes” or “not for human consumption” may still be sold directly to consumers with dosing instructions and may be of unknown quality or harmful [14].
This FDA warning was focused on unapproved GLP-1-related products, not Adipotide specifically, but the caution applies broadly to research-use marketing claims in weight-loss drug spaces [14]. Readers should not treat online claims as clinical evidence.
Where Published Data Remain Incomplete
Published Adipotide data remain incomplete for general human obesity care because there is no FDA-approved label, no established patient-selection framework, no validated long-term dosing regimen, and no robust published human efficacy program in the sources reviewed [8][10][11][17]. Long-term safety, reversibility of fat-tissue effects, renal monitoring thresholds, and vascular off-target risks remain important unanswered questions [2].
This does not make the compound uninteresting. It means the compound should be interpreted as experimental peptide research, not as a proven therapeutic option [1][2][8].
Side Effects and Safety Profile of Adipotide
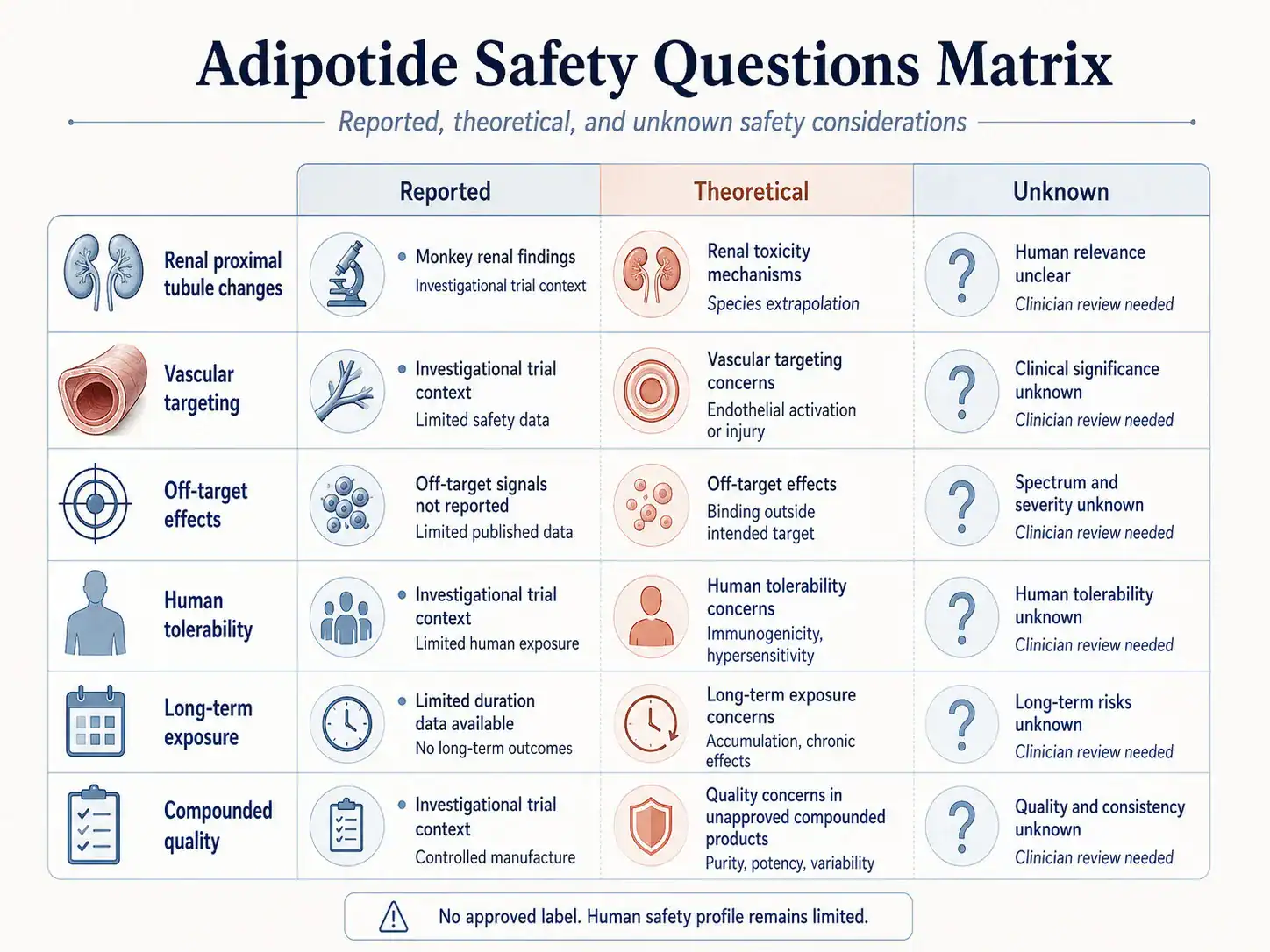
The safety profile of Adipotide is not established in the way it would be for an approved medication with prescribing information. The most cited safety concern in the preclinical literature is renal proximal tubule change in monkeys [2].
| Safety Area | What Is Known | Evidence Level | Practical Interpretation |
|---|---|---|---|
| Kidney findings | The primate study reported predictable and reversible renal proximal tubule changes at experimentally determined doses [2]. | Preclinical | Kidney safety is a key research concern; this is not a personal risk estimate. |
| Vascular effects | The intended mechanism targets blood vessels supplying white adipose tissue [1][2]. | Mechanistic/preclinical | Selectivity and off-target vascular effects require careful study. |
| Human tolerability | Phase 1 was designed to identify maximum tolerated dose and assess pharmacokinetics [8][10]. | Early human context | Public trial context does not equal an approved safety profile. |
| Long-term exposure | Long-term human safety and repeat-cycle safety are not established in approved labeling because no approved label was identified [17]. | Unknown | Long-term use claims should be treated as unsupported. |
| Product quality | FDA states compounded drugs are not FDA-approved and are not reviewed for safety, effectiveness, or quality before marketing 13. | Regulatory safety | Unapproved or compounded products add quality and oversight concerns. |
What Safety Findings Have Been Reported?
The main reported animal safety finding is dose-related renal proximal tubule change in monkeys, with changes described as predictable and reversible in the primate study [2]. The study also used renal function measures such as creatinine and kidney histology to assess toxicity [2].
In humans, the Phase 1 trial design focused on maximum tolerated dose, pharmacokinetics, weight change, and disease progression, but that design does not create an approved safety profile for general use [8][10].
Which Renal, Vascular, and Off-Target Safety Questions Remain?
Renal questions remain because kidney findings appeared in nonhuman primates, and any compound with renal toxicity signals requires careful clinical monitoring before broader use can be considered [2][11]. Vascular questions remain because the intended target is the blood vessel network supplying white adipose tissue, and vascular selectivity is central to the proposed therapeutic index [1][2].
Off-target questions also remain because prohibitin and annexin-related biology is not limited to a simple “fat cell receptor” story [1][4]. The more complex the target biology, the more important controlled safety assessment becomes [11].
Why Long-Term Safety Remains Unknown
Long-term safety remains unknown because published animal cycles and early human trial designs are not substitutes for large, longer-duration human trials [2][10][11]. Rare adverse events, long-term metabolic adaptation, kidney outcomes, vascular remodeling, and repeat-exposure risks are difficult to define without larger clinical programs [11].
Approved medicines usually include labeled warnings, adverse reactions, contraindications, and dosing instructions after regulatory review [15][16]. Adipotide does not have that approved-label framework in the public sources reviewed [8][17].
Contraindications, Drug Interactions, and Medical Supervision
There is no FDA-approved Adipotide label that lists formal contraindications or drug interactions [17]. Therefore, any discussion of contraindications is necessarily cautious and based on trial context, mechanism, and preclinical safety signals rather than approved prescribing information [1][2][8].
Who Might Require Extra Caution in Theory?
People with kidney disease, abnormal renal function, major vascular disease, cancer, pregnancy, breastfeeding, complex metabolic disease, or use of medications with renal or vascular effects would raise special theoretical concerns because Adipotide research involves renal findings and vascular targeting [1][2]. This is not a list of confirmed contraindications; it is a clinician-discussion framework based on evidence limits [2][11].
Practical clinician-discussion checklist:
- Current kidney function, kidney disease history, and nephrotoxic medication exposure [2].
- Cardiovascular and vascular disease history, given the vascular mechanism [1][2].
- Diabetes, prediabetes, insulin resistance, and glucose-lowering medication use [2][7].
- Cancer history or active cancer context, especially because the human trial involved advanced prostate cancer and obesity [8][10].
- Pregnancy, breastfeeding, fertility plans, and reproductive safety, because approved labeling is absent [17].
- Whether an FDA-approved obesity therapy or standard medical option is more appropriate [15][16].
- How to interpret animal data, early human evidence, and unsupported online claims [2][8][14].
What Interaction Questions Should Clinicians Consider?
No well-established Adipotide drug-interaction table exists in an FDA-approved label because no approved label was identified [17]. Clinicians evaluating peptide-related questions would logically focus on renal-risk medications, glucose-lowering therapies, blood-pressure or vascular medications, anticoagulants, and oncology therapies because these overlap with the compound’s preclinical safety signals and trial population [2][8][10].
This should not be interpreted as evidence that specific interactions have been proven. It is a safety-oriented framework for medical review when evidence is limited [11].
Dosage of Adipotide in Published Studies
Dosage information should be interpreted only as study context. Study doses are not personal dosing advice and should not be converted into self-use protocols.
What Dosage Has Been Used in Published Studies?
The 2011 primate study identified 0.43 mg/kg as the fixed subcutaneous daily dose used in the obese rhesus monkey efficacy study for 28 days, followed by a 28-day recovery period [2]. The same research program evaluated additional dose levels in nonhuman primate safety work, including 0.25, 0.43, and 0.75 mg/kg daily for 28 days [2].
The Phase 1 trial announcement stated that patients would receive Adipotide as an injection under the skin once daily for 28 days, with up to five dose levels tested and escalation based on observed safety [10]. This describes a supervised dose-escalation study design, not a recommended dosage for readers [10][11].
Why Study Dose Context Is Not Personal Dosing Advice
Animal doses do not translate directly into human self-dosing because species, body size, pharmacokinetics, toxicity thresholds, disease state, and monitoring requirements differ [2][11]. A Phase 1 maximum-tolerated-dose study is designed to find safety boundaries under clinical oversight, not to provide a public protocol [10][11].
Because Adipotide is not FDA-approved for obesity and no approved label was identified, there is no approved dose of Adipotide for personal weight-loss use [8][17]. Any online “dosage of Adipotide” claim should be treated as unsupported unless it is clearly tied to a cited study or official trial protocol [2][10].
Administration Routes Discussed in the Literature
Administration-route information is also study context. It should not be read as instructions for injection technique, reconstitution, storage, or self-administration.
Subcutaneous Administration as a Study Context
The primate study used subcutaneous daily administration in obese rhesus monkeys, including the fixed 0.43 mg/kg dose for 28 days [2]. The Phase 1 announcement similarly described under-the-skin injection once daily for 28 days in a clinical trial setting [10].
These details explain how Adipotide was studied. They do not establish that unsupervised use is safe, legal, effective, or medically appropriate [10][11][13].
Why Administration Details Are Not Self-Use Instructions
Administration details in clinical and preclinical papers are written for researchers and regulated clinical settings, not for self-use. FDA explains that an IND allows clinical research to proceed only after safety review intended to protect research subjects from unreasonable risk [11].
This article does not provide injection steps, mixing instructions, reconstitution guidance, cycle planning, or stacking suggestions. Those topics would be unsafe and inappropriate for an unapproved investigational compound [11][13].
Regulatory Status: Is Adipotide Peptide FDA-Approved?
Adipotide is not presented in the cited public record as an FDA-approved medication for obesity, diabetes, or cancer. The public record reviewed here describes an investigational compound, an IND/Phase 1 pathway, and a registered trial rather than an approved label [8][9][10][11].
How Investigational Status Differs From Approved Medical Use
An IND is not the same as FDA approval. FDA states that after an IND is submitted, the sponsor waits 30 calendar days before initiating clinical trials while FDA reviews the IND for safety to help ensure research subjects are not exposed to unreasonable risk [11].
FDA’s drug pages describe Drugs@FDA and the Orange Book as official resources for information about FDA-approved drug products and drug products approved on the basis of safety and effectiveness [17]. In contrast, Adipotide’s public development record is centered on investigational use and Phase 1 testing [8][9][10].
Risks of Unapproved, Compounded, or Research Peptide Use
FDA states that compounded drugs are not FDA-approved and that the agency does not verify their safety, effectiveness, or quality before marketing [13]. FDA has also warned that some unapproved weight-loss products are falsely labeled for research purposes or not for human consumption while being sold directly to consumers with dosing instructions, creating unknown quality and safety risks [14].
For Adipotide, this means a product marketed online as “research peptide” should not be assumed to match the compound used in published studies or regulated trials [2][10][14]. Product sourcing, identity, sterility, purity, dose accuracy, and legality are separate safety issues from the published scientific mechanism [13][14].
Adipotide vs Approved Obesity Therapies and Related Peptides
Adipotide comparisons are useful only when they clarify mechanism, evidence level, approval status, and safety. They should not be used to imply that Adipotide is better, safer, or appropriate for personal use.
Adipotide vs GLP-1 and GIP-Based Anti-Obesity Medications
Adipotide’s proposed mechanism is adipose-vascular targeting, while FDA-approved obesity medications such as semaglutide and tirzepatide act through incretin-related pathways and have approved indications in defined populations [1][15][16]. FDA approved tirzepatide injection for chronic weight management in adults with obesity or overweight with at least one weight-related condition, used with reduced-calorie diet and increased physical activity [15].
Wegovy labeling describes semaglutide as indicated to reduce excess body weight and maintain weight reduction long term in specified adults and pediatric patients, and also includes other approved indications depending on formulation and population [16]. This approved-label status is the key difference: semaglutide and tirzepatide products have regulatory review, labeling, and defined safety information, while Adipotide remains investigational in the public record [8][15][16].
How Adipotide Differs From General Metabolic Peptides
A review of anti-obesity peptides and peptidomimetics discusses multiple peptide-based strategies, including GLP-1-related, melanocortin-related, and other metabolic pathways 20. Adipotide is distinct because it is not primarily a gut-hormone mimetic or appetite peptide; it is a targeted proapoptotic peptide aimed at adipose vasculature [1][2].
That distinction is scientifically interesting but safety-sensitive. A peptide that targets tissue vasculature has a different risk profile than a peptide designed to modulate appetite, insulin secretion, or satiety signaling [1][2][15][16].
Key Takeaways for Interpreting Adipotide Research
The safest way to interpret Adipotide is through evidence quality, regulatory status, and safety data. It is an experimental peptide with a defined target concept and notable preclinical findings, but not an approved obesity medication with established human benefits, dosing, or long-term safety [1][2][8][11].
For readers considering peptide-related medical decisions, the most useful next step is not to seek a protocol. It is to discuss evidence quality, kidney and vascular safety questions, approved alternatives, current medications, and regulatory status with a qualified healthcare professional [2][13][15][16].
Researchers Cited in This Article
The researchers below authored or co-authored publications cited in this article. Listing them here identifies sources; it does not mean they wrote, independently reviewed, sponsored, or endorsed this PeptideDosages.com article. The site author is identified in the article byline.
Mikhail G. Kolonin
Researcher profile: McGovern Medical School
Mikhail G. Kolonin’s published work is directly relevant to the adipose-vascular research lane behind Adipotide peptide. His preclinical publications helped frame white adipose tissue as a vascularly supported biological system and explored how targeted interventions in adipose tissue models may affect obesity-related outcomes. His review work also provides useful pharmacology and published literature context for interpreting vascular targeting as an experimental concept, not as established human treatment. This background is especially relevant to the article’s focus on mechanism, preclinical evidence, evidence limitations, and the distinction between animal findings and clinical use.
Selected publications:
- Reversal of obesity by targeted ablation of adipose tissue — Nature Medicine, 2004. DOI: 10.1038/nm1048. PMID: 15133506.
- Vascular targeting of adipose tissue as an anti-obesity approach — Trends in Pharmacological Sciences, 2011. DOI: 10.1016/j.tips.2011.01.004. PMID: 21349592.
Renata Pasqualini
Researcher profile: Research with Rutgers
Renata Pasqualini’s publications are relevant to ligand-directed peptide research, vascular targeting, and the receptor biology discussed in this Adipotide article. Her coauthored work on the obese-monkey Adipotide study provides context for the article’s preclinical evidence discussion, including white-fat targeting, insulin-resistance markers, and renal safety signals. Her related work on prohibitin and annexin A2 helps support a more cautious mechanism-of-action discussion by showing that adipose tissue targeting involves complex endothelial and adipocyte biology rather than a simple consumer-facing “fat loss” claim.
Selected publications:
- A Peptidomimetic Targeting White Fat Causes Weight Loss and Improved Insulin Resistance in Obese Monkeys — Science Translational Medicine, 2011. DOI: 10.1126/scitranslmed.3002621. PMID: 22072637.
- Prohibitin/annexin 2 interaction regulates fatty acid transport in adipose tissue — JCI Insight, 2016. DOI: 10.1172/jci.insight.86351. PMID: 27468426.
Related dosage protocols and research
Use the available links to move between research context, dosage pages or comparisons, and supporting guides. When vial-size variants exist, they remain separate because concentration and syringe-unit calculations change with vial strength. Comparisons do not imply that different compounds are interchangeable.
Matching dosage protocols
Further research context
REFERENCES
- National Cancer Institute. Prohibitin-targeting peptide 1. NCI Drug Dictionary. Accessed 2026.
- Barnhart KF, Christianson DR, Hanley PW, et al. A peptidomimetic targeting white fat causes weight loss and improved insulin resistance in obese monkeys. Science Translational Medicine. 2011;3(108):108ra112. doi:10.1126/scitranslmed.3002621. PMID: 22072637.
- Kolonin MG, Saha PK, Chan L, Pasqualini R, Arap W. Reversal of obesity by targeted ablation of adipose tissue. Nature Medicine. 2004;10(6):625-632. doi:10.1038/nm1048. PMID: 15133506.
- Salameh A, Daquinag AC, Staquicini DI, et al. Prohibitin/annexin 2 interaction regulates fatty acid transport in adipose tissue. JCI Insight. 2016;1(10):e86351. doi:10.1172/jci.insight.86351. PMID: 27468426.
- Rupnick MA, Panigrahy D, Zhang CY, et al. Adipose tissue mass can be regulated through the vasculature. Proceedings of the National Academy of Sciences. 2002;99(16):10730-10735. doi:10.1073/pnas.162349799. PMID: 12149466.
- Kim DH, Woods SC, Seeley RJ. Peptide designed to elicit apoptosis in adipose tissue endothelium reduces food intake and body weight. Diabetes. 2010;59(4):907-915. doi:10.2337/db09-1141. PMID: 20103704.
- Kim DH, Sartor MA, Bain JR, et al. Rapid and weight-independent improvement of glucose tolerance induced by a peptide designed to elicit apoptosis in adipose tissue endothelium. Diabetes. 2012;61(9):2299-2310. doi:10.2337/db11-1579. PMID: 22733798.
- ClinicalTrials.gov. A First-in-Man, Phase I Evaluation of a Single Cycle of Prohibitin Targeting Peptide 1 in Patients With Metastatic Prostate Cancer and Obesity. NCT01262664. ClinicalTrials.gov.
- Arrowhead Pharmaceuticals. Arrowhead Announces FDA Clearance to Initiate Adipotide Phase I Clinical Trial. Press release. 2012.
- Arrowhead Pharmaceuticals. Arrowhead Announces Dosing of First Patient with Anti-Obesity Treatment Adipotide in a Phase 1 Clinical Trial. Press release. 2012.
- U.S. Food and Drug Administration. Investigational New Drug (IND) Application. FDA. Updated 2025.
- Centers for Disease Control and Prevention. Adult Obesity Facts. CDC. Updated 2024.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. FDA. Updated 2025.
- U.S. Food and Drug Administration. FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss. FDA. Updated 2026.
- U.S. Food and Drug Administration. FDA Approves New Medication for Chronic Weight Management. FDA Press Announcement. 2023.
- U.S. Food and Drug Administration. WEGOVY prescribing information. FDA-approved labeling. 2025.
- U.S. Food and Drug Administration. Drugs. FDA drug information and database portal, including Drugs@FDA and Orange Book resources. Accessed 2026.
- Criscione L. Comment on “A peptidomimetic targeting white fat causes weight loss and improved insulin resistance in obese monkeys”. Science Translational Medicine. 2012;4(125):125le1. PMID: 22539771.
- Barnhart KF, et al. Response to Comment on “A Peptidomimetic Targeting White Fat Causes Weight Loss and Improved Insulin Resistance in Obese Monkeys”. Science Translational Medicine. 2012. doi:10.1126/scitranslmed.3004103.
- Kumar MS, et al. Peptides and peptidomimetics as potential antiobesity agents. Frontiers in Nutrition. 2019;6:11. doi:10.3389/fnut.2019.00011.