
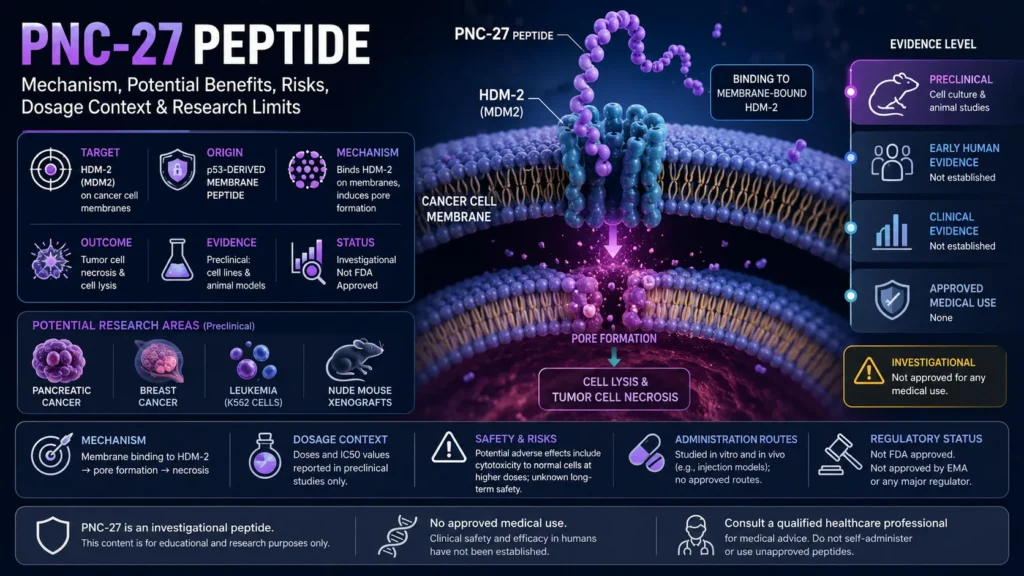
PNC-27 peptide is an investigational, p53-derived peptide described by the National Cancer Institute as a synthetic agent with potential antineoplastic activity and a proposed ability to interact with HDM-2 on cancer cell membranes 1. This educational article reviews what researchers have studied about PNC-27, including its proposed HDM-2 membrane mechanism, potential benefits, evidence limits, side effects, dosage context, administration routes in the literature, and regulatory status. It is not a treatment recommendation, dosing protocol, or substitute for oncology care.
Key points:
- PNC-27 is a research-stage peptide, not an approved cancer drug. Public FDA drug databases do not list an approved PNC-27 product or labeled indication when searched by name 14, 15.
- Its scientific rationale comes from p53 and HDM-2 biology. p53 is encoded by TP53, and MDM2/HDM-2 is a major p53-regulating protein in cancer biology 5, 6.
- The main proposed mechanism is preclinical. PNC-27 is described as binding HDM-2 associated with cancer cell membranes and inducing membrane disruption or pore formation in tumor cells [1], 3.
- Evidence is mostly laboratory-based. PubMed-indexed PNC-27 literature is limited and appears centered on mechanistic, cancer cell line, and animal-model research rather than large human trials 2, 16.
- Potential benefits should be interpreted cautiously. Claims about PNC-27 killing cancer cells refer to preclinical endpoints such as cancer cell cytotoxicity, cell lysis, or tumor cell necrosis, not proven patient outcomes [1], [2], [3].
- Human safety, side effects, contraindications, interactions, pharmacokinetics, and dosing are not established. Study concentrations or animal-model exposure should not be converted into personal dosing advice [14], [15], [16].
- Regulatory status matters. Unapproved or compounded peptide products are not evaluated the same way as FDA-approved drugs, and FDA materials emphasize that compounded drugs do not undergo FDA premarket review for safety, effectiveness, or manufacturing quality 17, 18.
Fast Answer
PNC-27 peptide is an investigational p53-derived anti-cancer peptide studied mainly for its proposed interaction with HDM-2 on the cancer cell membrane and possible pore formation leading to tumor cell necrosis [1], [3]. People search for it because preclinical papers discuss PNC-27 killing cancer cells, but that does not prove human cancer benefit [2], [16]. No approved label dose, FDA-approved indication, or standard clinical protocol is established [14], [15]. Safety questions require oncology supervision.
What Is the PNC-27 Peptide?
PNC-27 is a synthetic peptide discussed in cancer research because it combines a p53-derived HDM-2-binding concept with membrane-targeting behavior described by the National Cancer Institute [1]. It is best understood as an investigational anti-cancer peptide candidate, not as an approved therapy for pancreatic cancer, breast cancer, leukemia, cervical cancer, or any other neoplasm [14], [15], [16].
The naming can be confusing because older PNC-27 papers often use HDM-2, while modern protein databases commonly use MDM2 for the human MDM2 proto-oncogene protein [6]. This article uses HDM-2 when discussing the PNC-27 literature and MDM2 when discussing broader p53 biology.
PNC-27 as a p53-Derived Anti-Cancer Peptide
PNC-27 is described as a p53-derived peptide because its proposed cancer-cell interaction relates to the region of p53 that can bind HDM-2/MDM2 [1]. p53 itself is a tumor-suppressor protein encoded by TP53, and it plays central roles in cell-cycle control, DNA-damage response, apoptosis, and cancer biology [5].
MDM2/HDM-2 is important because it binds p53 and suppresses p53-mediated transcriptional activity, a relationship first characterized in foundational molecular oncology studies 7. Structural work later showed how a p53 transactivation-domain peptide binds a pocket on the MDM2 oncoprotein, helping explain why this interaction became a target in anti-cancer drug discovery 8.
Basic Structure: p53 Binding Domain Plus Membrane Residency Peptide
The NCI Drug Dictionary describes PNC-27 as a synthetic peptide containing an HDM-2-binding domain from p53 linked to a membrane residency peptide, with proposed antineoplastic activity [1]. That structure is meant to explain why researchers discuss PNC-27 as a membrane-active peptide that binds HDM-2 associated with cancer cell membranes rather than only as a classic intracellular p53-reactivating compound [1], [3].
The phrase membrane residency peptide should not be interpreted as a verified human pharmacology claim. It describes how the compound was designed and studied in preclinical systems, not an approved route, dose, biodistribution pattern, or patient-level safety profile [1], [14], [16].
How Does PNC-27 Differ From Approved Peptide Drugs?
Approved peptide drugs have regulator-reviewed prescribing information, labeled indications, manufacturing standards, contraindications, warnings, adverse-event data, and dosage instructions for specific populations [14], [15]. PNC-27 does not have those features in FDA public approval databases, so it should be framed as investigational and evidence-limited [14], [15].
This distinction is practical. A peptide can be biologically interesting in cell biology while still lacking the clinical evidence, quality controls, pharmacokinetic data, and safety documentation required for routine medical use [16], [17], [18].
Why Is PNC-27 Studied in Cancer Cell Research?
PNC-27 is studied because some preclinical reports describe cancer cell membrane-associated HDM-2 and a possible selective cytotoxic effect of PNC-27 on tumor cells [1], [2], [3]. In this model, the peptide binds to HDM-2 in the cancer cell membrane, contributes to membrane disruption, and may induce tumor cell necrosis through pore formation [1], [3].
That mechanism is interesting, but it remains a research hypothesis until confirmed by stronger human evidence. Cell-line studies and animal models can generate hypotheses, but they cannot establish that a peptide improves survival, shrinks tumors, prevents recurrence, or is safe in people with cancer [16], 22.
Why Target Tumor Cells Rather Than Normal Cells?
Selective toxicity is a major goal in oncology: researchers want cancer therapies to damage tumor cells more than normal cells. PNC-27 literature discusses possible selectivity because some cancer cells may express HDM-2 in their membranes, while normal or untransformed cell line models are described differently in preclinical reports [1], [2], [3].
However, selectivity in a dish is not the same as a safe therapeutic window in humans. Human tumors are heterogeneous, normal tissues vary, drug exposure differs by organ, and systemic toxicity may not appear in simplified cancer cell line experiments [16], [22].
Why Does HDM-2 in Cancer Cell Membranes Matter?
HDM-2 matters because the PNC-27 model depends on a cell-surface or membrane-associated target rather than only intracellular p53 regulation [1]. MDM2 is best known for controlling p53 stability and activity, including p53 degradation pathways described in major p53-MDM2 studies 9, 10.
If HDM-2 is present in the membrane of cancer cells, a membrane-active peptide could theoretically bind there and disturb the cell membrane [1], [3]. The key uncertainty is whether this membrane expression pattern, binding event, and cell death mechanism translate reliably across human cancers and patient conditions [2], [16].
How Does PNC-27 Peptide Work?
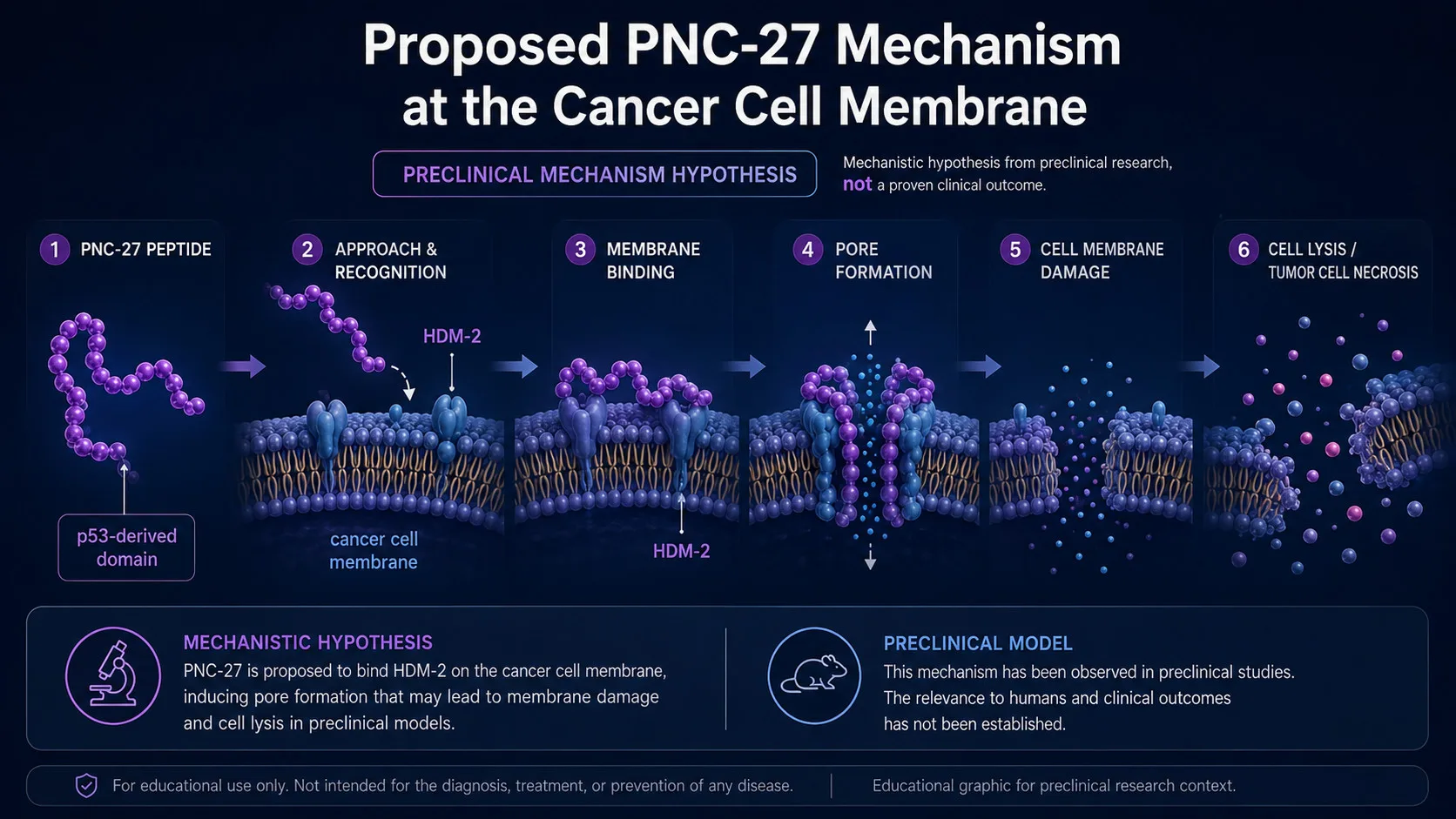
The proposed mechanism is that PNC-27 binds HDM-2 associated with the cancer cell membrane and triggers membrane damage, pore formation, cell lysis, and tumor cell necrosis [1], [3]. This is a preclinical mechanism-of-action model, not proof that PNC-27 peptide is an effective cancer treatment in humans [16], [22].
A useful way to read the literature is to separate mechanism, model, and medical outcome. Mechanism describes what may happen in cells; model describes where it was tested; medical outcome requires human data such as tumor response, progression-free survival, overall survival, adverse events, and quality-of-life endpoints [16], [22].
How Is PNC-27 Proposed to Bind HDM-2?
PNC-27 contains a p53-related HDM-2-binding component, and the p53-MDM2 interface is a well-studied protein-protein interaction in cancer biology [1], [8]. In structural studies of MDM2, a p53 transactivation-domain peptide binds a defined hydrophobic pocket on MDM2, which helped inspire several MDM2-targeting drug-discovery strategies [8], 11.
For PNC-27, the proposed binding event is described at HDM-2 associated with the cancer cell membrane [1], [3]. That makes PNC-27 different from small-molecule MDM2 antagonists, which were designed mainly to disrupt intracellular p53-MDM2 binding and reactivate p53 signaling [11], 12.
How Might Cancer Cell Membrane Disruption and Pore Formation Occur?
PNC-27 is described as a membrane-active peptide, meaning its proposed cytotoxic effect involves cancer cell membrane disruption rather than only intracellular signaling [1], [3]. Reviews of anticancer peptides note that some peptide-based molecules can interact with tumor cell membranes, alter membrane integrity, and cause cytotoxicity in preclinical systems, but these effects depend heavily on peptide chemistry, membrane composition, model system, and exposure conditions 13.
In the PNC-27 model, transmembrane pore formation is proposed after interaction of PNC-27 with HDM-2 on the membrane of cancer cells [1], [3]. That concept should be interpreted as a laboratory mechanism until supported by clinical pharmacology, biodistribution, and human safety data [16], [22].
Why Mechanism Does Not Prove Clinical Benefit
A plausible mechanism does not establish that a drug improves human outcomes. Many anti-cancer candidates look active in cancer cell lines or animal models but fail because of toxicity, poor pharmacokinetics, tumor heterogeneity, immune effects, resistance mechanisms, or lack of clinical efficacy [16], [22].
For PNC-27, the most responsible interpretation is that preclinical findings support further research, not self-treatment. Without an approved indication, label dose, human safety profile, or well-designed clinical trials, claims about patient benefit remain unproven [14], [15], [16].
PNC-27 and HDM-2: Membrane Mechanism in Detail
The distinctive feature of the PNC-27 hypothesis is the interaction between PNC-27 and HDM-2 in cancer cell membranes [1], [3]. This is different from the broader p53-MDM2 field, where much of the research focuses on intracellular MDM2 regulation of p53 and small molecules that block that interaction [11], [12].
The mechanism is sometimes summarized too strongly online. A safer evidence-based summary is: published preclinical sources suggest that PNC-27 may bind membrane-associated HDM-2 on some cancer cells and induce membrane damage, but clinical relevance is not established [1], [2], [3], [16].
How Is Membrane-Bound HDM-2 Different From Intracellular HDM-2?
Intracellular MDM2 is a major negative regulator of p53, including pathways that lead to p53 suppression or degradation [7], [9], [10]. Membrane-bound HDM-2, as discussed in PNC-27 literature, is proposed to act as a surface-associated binding target that can bring the peptide to the cancer cell membrane [1], [3].
This difference matters because the biological outcome may differ. Blocking intracellular MDM2 can reactivate p53 signaling in some contexts, while membrane interaction with PNC-27 is proposed to cause cell membrane damage, pore formation, and necrosis [1], [11], [12].
How Might the PNC-27–HDM-2 Interaction Cause Transmembrane Pore Formation?
The proposed sequence is: PNC-27 binds HDM-2 associated with the cancer cell membrane, localizes to that membrane, and contributes to structural disruption that produces pores in the cancer cell [1], [3]. Those pores are hypothesized to compromise membrane integrity, leading to cell lysis and necrotic tumor cell death [1], [3].
The model is biologically plausible within preclinical membrane-active peptide research, but it remains evidence-limited. Human tumors, blood plasma proteins, immune clearance, tissue penetration, and peptide stability can all affect whether a membrane mechanism seen in vitro occurs in patients [13], [16], [22].
Necrosis, Cell Lysis, and Cell Death Pathways
PNC-27 is often described as inducing tumor cell necrosis rather than primarily triggering p53-dependent apoptosis [1], [3]. Necrosis in this context refers to cell death linked to membrane injury and cell lysis, while apoptosis is a more regulated cell death pathway often discussed in p53 signaling and MDM2-inhibition research [11], [12].
That distinction can help readers interpret “PNC-27 kills” language. It refers to preclinical observations of cytotoxicity or cell death in cancer cell models, not a confirmed clinical cancer response [1], [2], [3], [16].
What Is PNC-27 Used For in Research?
PNC-27 is used in research to study cancer cell membrane targeting, HDM-2-related binding, peptide-induced pore formation, and cytotoxicity in tumor cell models [1], [2], [3]. It is not FDA-approved for cancer treatment, cancer prevention, supportive oncology care, or any non-cancer indication [14], [15].
The most relevant use category is preclinical oncology research. That includes cancer cell line experiments, mechanistic cell biology, and animal-model studies that test whether the peptide can affect tumor cells under controlled conditions [2], [3], [16].
Cancer Cell Lines Studied, Including Pancreatic and Breast Cancer
PNC-27 literature and database searches include terms related to human pancreatic cancer cells, human breast cancer cells, leukemia-related cell lines such as K562 cells, and other cancer cell models [2], [3]. These are important research tools, but a human-derived cancer cell line is not the same as a clinical study in people with cancer [16], [22].
A cell line can help researchers measure cytotoxicity, HDM-2 expression, colocalization of PNC-27 with HDM-2, membrane disruption, and IC50-like dose-response metrics [2], [3]. It cannot show whether PNC-27 improves overall survival, reduces metastatic spread, or is tolerable in patients receiving chemotherapy, immunotherapy, surgery, or radiation [16], 20, 21.
What “PNC-27 kills” Means in Cancer Cell Studies
When a paper or summary says “PNC-27 kills” cancer cells, the phrase should be read in laboratory context. It usually means cancer cells treated with PNC-27 showed reduced viability, cell membrane damage, cell lysis, or tumor cell necrosis under experimental conditions [1], [2], [3].
It does not mean PNC-27 cures cancer, works for every cancer cell line, selectively spares all normal cells, or has proven human efficacy. Those claims require clinical trials with defined endpoints, dosing, safety monitoring, comparator groups, and follow-up [16], [22].
Potential Benefits of PNC-27: What Is Supported?
The potential benefits of PNC-27 are mainly hypothesis-generating: possible cancer cell selectivity, possible membrane-targeted cytotoxicity, and a mechanism that differs from conventional p53-reactivation approaches [1], [3], [11]. None of these potential benefits has been established as an approved medical use or standard clinical oncology benefit [14], [15], [16].
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| Compound identity | NCI describes PNC-27 as a synthetic p53-derived peptide with a membrane residency peptide and potential antineoplastic activity [1]. | Preclinical / investigational | Supports what PNC-27 is; does not establish approved use. |
| HDM-2 membrane mechanism | PNC-27 is described as interacting with HDM-2 associated with cancer cell membranes and inducing pore formation [1], [3]. | Preclinical | Supports a proposed mechanism; does not prove human outcomes. |
| Cancer cell cytotoxicity | PubMed-indexed PNC-27 literature discusses cancer cell lines, cytotoxicity, and tumor cell necrosis [2], [3]. | Preclinical | Shows laboratory activity; cannot determine patient benefit. |
| Animal-model activity | PNC-27 searches identify preclinical animal-model context, but these studies remain translational evidence [2]. | Preclinical | Can guide hypotheses; cannot set human dose or safety. |
| Human clinical benefit | A direct ClinicalTrials.gov search by name does not identify an established PNC-27 clinical trial record at article preparation [16]. | Not established | Does not support treatment claims. |
| Approved use | FDA public approval databases do not list an approved PNC-27 drug product when searched by name [14], [15]. | No approved medical use identified | No approved label dose, indication, or prescribing information. |
Possible Selectivity for Cancer Cells Over Normal Cells
PNC-27 is discussed as potentially selective because the proposed target is HDM-2 in cancer cell membranes, and some preclinical reports compare cancer cells with normal cells or untransformed cell line models [1], [2], [3]. This is one reason PNC-27 is described as an anti-cancer peptide candidate rather than a general membrane toxin [1].
Still, selectivity must be proven in living systems. Normal human tissues, epithelial cells, blood components, immune cells, and organ systems may behave differently from simplified culture models, and the absence of toxicity in one preclinical model cannot rule out human adverse events [16], [17], [22].
Potential Anti-Cancer Effects Still Require Clinical Testing
Potential anti-cancer effects include cancer cell membrane disruption, tumor cell necrosis, and cytotoxicity to cancer cells in preclinical settings [1], [2], [3]. These effects are not the same as a verified treatment effect in pancreatic cancer, breast cancer, cervical cancer, leukemia, or other patient populations [16], [22].
Clinical testing would need to define route, dose, pharmacokinetics, toxicity, tumor type, inclusion criteria, endpoints, and interactions with standard care. Until that evidence exists, PNC-27 should be discussed as an investigational peptide with unproven clinical benefit [14], [16].
What Does Human Research Show About PNC-27?
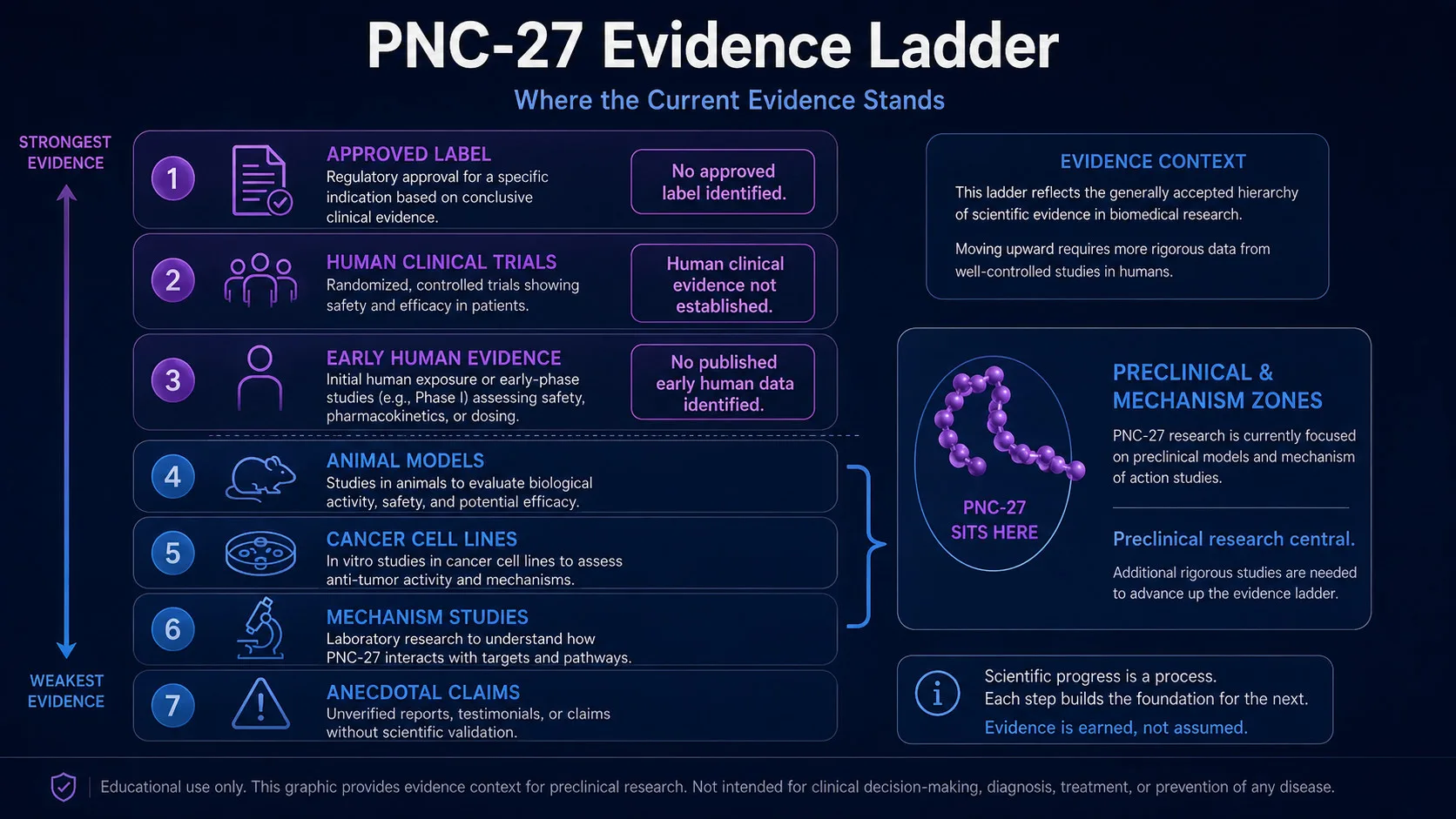
Human evidence for PNC-27 appears very limited. Public searches of PubMed and ClinicalTrials.gov by the term PNC-27 identify a small research footprint and do not show an established, regulator-reviewed, FDA-approved clinical use or labeled human dosing program [2], [14], [15], [16].
This does not mean the science is uninteresting. It means the evidence hierarchy is low for clinical decision-making, because human efficacy and safety require well-designed clinical studies, not only mechanistic papers, cell line experiments, or animal models [16], [22].
Current Status of Clinical Evidence and Human Trials
At the time this article was prepared, a direct ClinicalTrials.gov search for PNC-27 did not identify a registered study record by that name [16]. Public FDA databases also do not show an approved PNC-27 product with prescribing information, which means there is no approved label dose or FDA-reviewed indication [14], [15].
If future clinical trials are registered, readers should look for trial phase, cancer type, eligibility criteria, route of administration, dose-escalation design, adverse-event reporting, tumor response endpoints, and whether results are peer-reviewed. ClinicalTrials.gov explains that clinical studies are designed to evaluate health interventions in human participants, which is different from cell or animal research [22].
Why Case Reports or Anecdotes Cannot Establish Efficacy
Anecdotes and online reports cannot show whether a cancer response was caused by PNC-27, another treatment, natural disease variation, imaging interpretation, selection bias, or reporting bias. Human clinical evidence needs defined protocols, safety monitoring, endpoints, and preferably controlled designs [16], [22].
This is especially important in oncology. Delaying evidence-based treatment for an unapproved peptide could affect outcomes, and standard cancer treatments such as chemotherapy and immunotherapy have defined clinical roles, risks, and monitoring requirements [20], [21].
What Does Preclinical Research Show in Cancer Cell Lines?
Preclinical PNC-27 research centers on cancer cell lines, HDM-2 membrane localization, cytotoxicity, cell lysis, and tumor cell necrosis [1], [2], [3]. These models are useful for understanding how a peptide might affect a cancer cell membrane, but they are not designed to establish human benefit [16], [22].
The important editorial distinction is that human-derived cells are not the same as human evidence. Human pancreatic cancer cells in a dish can help study mechanism; they do not provide clinical dosing, side-effect rates, drug interaction data, or survival outcomes [2], [16].
In Vitro Findings Across Different Cancer Cell Lines
In vitro PNC-27 studies have examined different cancer cell lines and reported cytotoxic effects under controlled laboratory conditions [2], [3]. Researchers may use different concentrations of PNC-27, viability assays, microscopy, HDM-2 antibody staining, and IC50-like calculations to understand the effect of PNC-27 on cancer cells [2], [3].
Those measurements are not personal dosing instructions. IC50 values and cell-culture concentrations describe experimental exposure in a controlled system, not an approved therapeutic dose, route, frequency, or safety margin in humans [16], [22].
Control Peptide PNC-29 and Negative Control Comparisons
The PNC-27 research context includes comparison peptides such as the control peptide PNC-29, which is discussed as a negative control peptide in relation to PNC-27’s proposed mechanism [2], [3]. Control peptides are important because they help researchers test whether a cytotoxic effect depends on a specific structure of PNC-27 rather than nonspecific peptide exposure [2], [3].
A useful study-design question is whether the whole peptide, p53-derived domain, membrane residency domain, and control peptide show different effects. Those comparisons help interpret binding of PNC-27, interaction of PNC-27 with HDM-2, and whether the effect is specific enough to justify further translational work [1], [2], [3].
What Have Animal Models Suggested About PNC-27?
Animal models can test questions that cell culture cannot, including tumor growth, systemic exposure, tissue distribution, and observable toxicity under controlled conditions. PNC-27 searches identify preclinical literature that includes animal-model context, but these findings remain preclinical and cannot establish clinical efficacy in humans [2], [16], [22].
Animal studies are valuable when they are well-designed, reproducible, and interpreted cautiously. They are not substitutes for human dose-escalation studies, pharmacokinetics, adverse-event monitoring, or oncology outcomes [16], [22].
Nude Mouse Xenograft Findings and Translational Limits
Nude mouse xenograft studies are commonly used in oncology research because human tumor cells can be implanted into immunodeficient mice, allowing researchers to study tumor growth under experimental conditions. PNC-27-related searches include nude mouse and xenograft terminology, but these models lack the full human immune context and cannot predict all human toxicities or responses [2], [16], [22].
The translational limit is especially relevant for a membrane-active anti-cancer peptide. Peptide stability, blood plasma binding, immune recognition, organ distribution, tumor penetration, and off-target membrane interactions may differ between mice and humans [13], [16], [22].
Side Effects and Safety Concerns for PNC-27
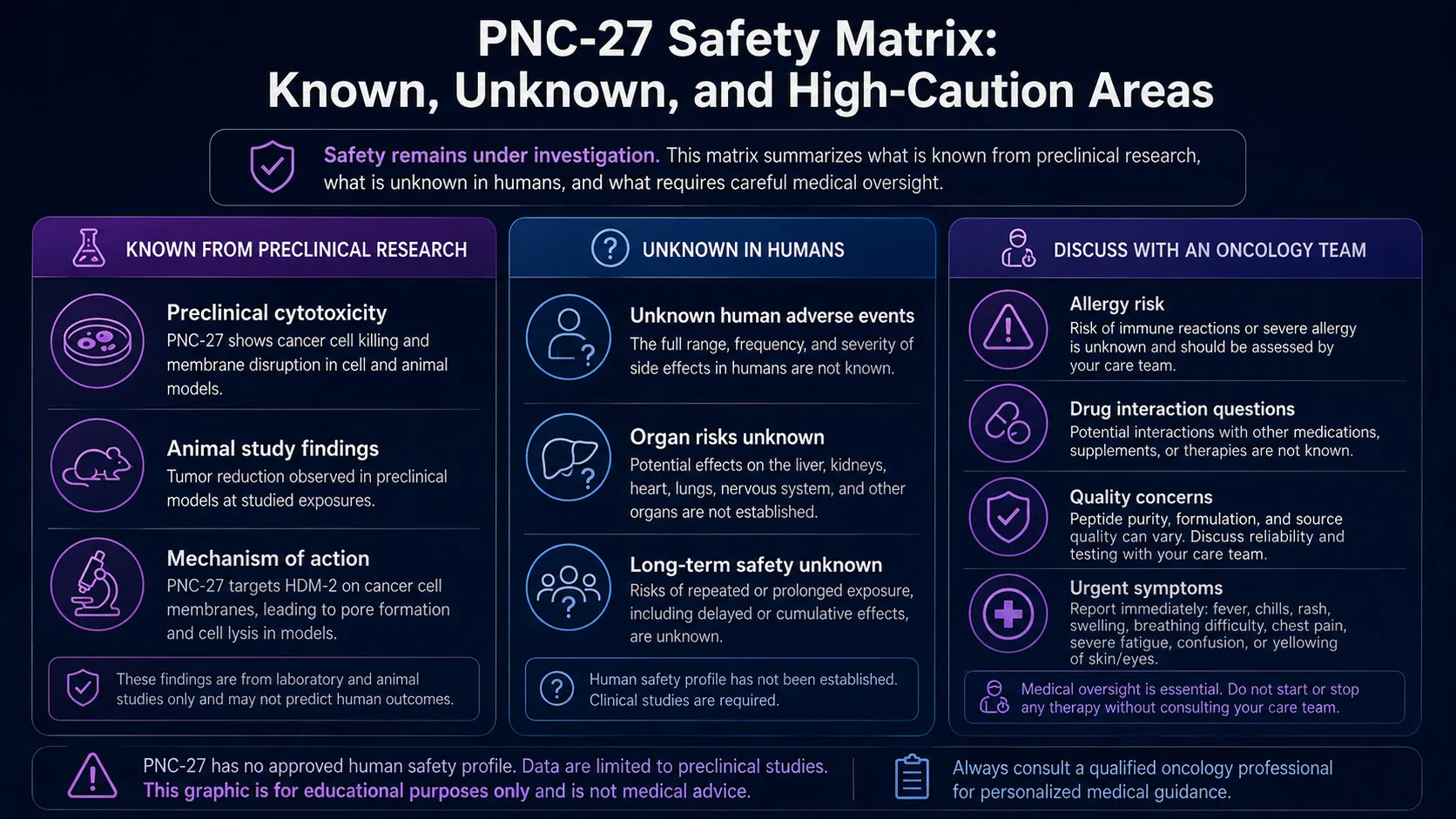
There is no established human adverse-event profile for PNC-27 in an FDA-approved label because no FDA-approved PNC-27 product is listed in public approval databases [14], [15]. That means side effects, serious adverse events, contraindications, overdose risks, drug interactions, pregnancy and breastfeeding risks, and long-term safety remain inadequately characterized for clinical use [14], [15], [16].
For unapproved or compounded peptide products, safety concerns also include identity, purity, sterility, potency, contamination, labeling, and manufacturing quality. FDA materials explain that compounded drugs are not FDA-approved and are not reviewed by FDA for safety, effectiveness, or quality before marketing [17].
What Is Known From Preclinical Cytotoxicity Studies?
Preclinical PNC-27 studies focus on cytotoxicity to cancer cells, possible selectivity compared with normal cells, and membrane-associated HDM-2 mechanisms [1], [2], [3]. Those findings are relevant to research, but they do not establish a human safety profile or rule out harm to normal tissues [16], [22].
A peptide that damages cancer cell membranes could still have off-target effects if it reaches normal tissues, blood components, or organs in sufficient exposure. That risk cannot be assessed fully without human pharmacology and safety studies [16], [17], [22].
Unknown Human Adverse Events, Allergic Reactions, and Organ Risks
Unknown risks include allergic reactions, immune responses, injection-site complications if a parenteral route were ever studied, organ toxicity, blood or bone marrow effects, and interactions with cancer therapies, but these risks have not been quantified in an approved PNC-27 label [14], [15], [16]. The absence of label-reported adverse reactions is not evidence that the peptide is safe; it reflects the absence of an approved product and established clinical safety dataset [14], [15].
Any severe symptom during cancer care, such as bleeding, hematemesis, fever, severe pain, shortness of breath, confusion, or allergic reaction, requires urgent medical evaluation. That statement reflects standard medical caution rather than a PNC-27-specific adverse-event profile, because PNC-27-specific human safety data are not established [14], [16], [20], [21].
Why Cancer Patients Need Oncology Supervision
Cancer treatment decisions depend on diagnosis, stage, tumor biology, performance status, comorbidities, goals of care, and the evidence supporting available treatments. NCI materials describe chemotherapy and immunotherapy as established cancer treatment categories with defined indications, risks, and monitoring needs [20], [21].
PNC-27 should not replace evidence-based oncology care. A person with cancer should discuss investigational claims, clinical trial options, medication interactions, and risks of unapproved products with an oncology team [16], [17], [20], [21].
Contraindications, Drug Interactions, and Medical Supervision
Formal contraindications for PNC-27 are not established in FDA-approved prescribing information because there is no approved PNC-27 label [14], [15]. In practice, that means clinicians would need to consider uncertainty itself as a safety issue, especially in people with cancer, pregnancy, breastfeeding, immune compromise, organ dysfunction, bleeding risk, or complex medication regimens [14], [16], [17].
Drug interactions are also not well characterized. Without human pharmacokinetic and safety studies, it is not possible to define how PNC-27 might interact with chemotherapy, immunotherapy, targeted therapy, radiation, anticoagulants, corticosteroids, antiemetics, antibiotics, or supportive-care medications [16], [20], [21].
Contraindications That Would Require Clinician Review
Clinician review would be especially important for people receiving active cancer treatment, people with severe liver or kidney disease, people with immune suppression, people with a history of severe allergic reactions, and people who are pregnant or breastfeeding. These categories require caution because PNC-27 lacks approved prescribing information and human safety data [14], [15], [16], [17].
A clinician would also need to consider whether an investigational peptide could interfere with standard treatment timing, trial eligibility, laboratory interpretation, or adverse-event attribution. Those questions are central in oncology research and clinical care [16], [20], [21], [22].
Potential Interactions With Chemotherapy, Immunotherapy, and Supportive Care
Chemotherapy and immunotherapy can have significant toxicities and must be managed in a structured medical context [20], [21]. Because PNC-27 has no established interaction profile, combining it with cancer treatments outside a regulated research protocol would create unknown safety and interpretive risks [16], [17], [20], [21].
Supportive-care drugs also matter. Anticoagulants, steroids, antiemetics, analgesics, growth factors, antibiotics, and supplements may affect bleeding, immune response, metabolism, or symptom interpretation, and unstudied peptide exposure could complicate clinical decisions [16], [17], [20], [21].
What Dosage Information Exists for PNC-27 Peptide?
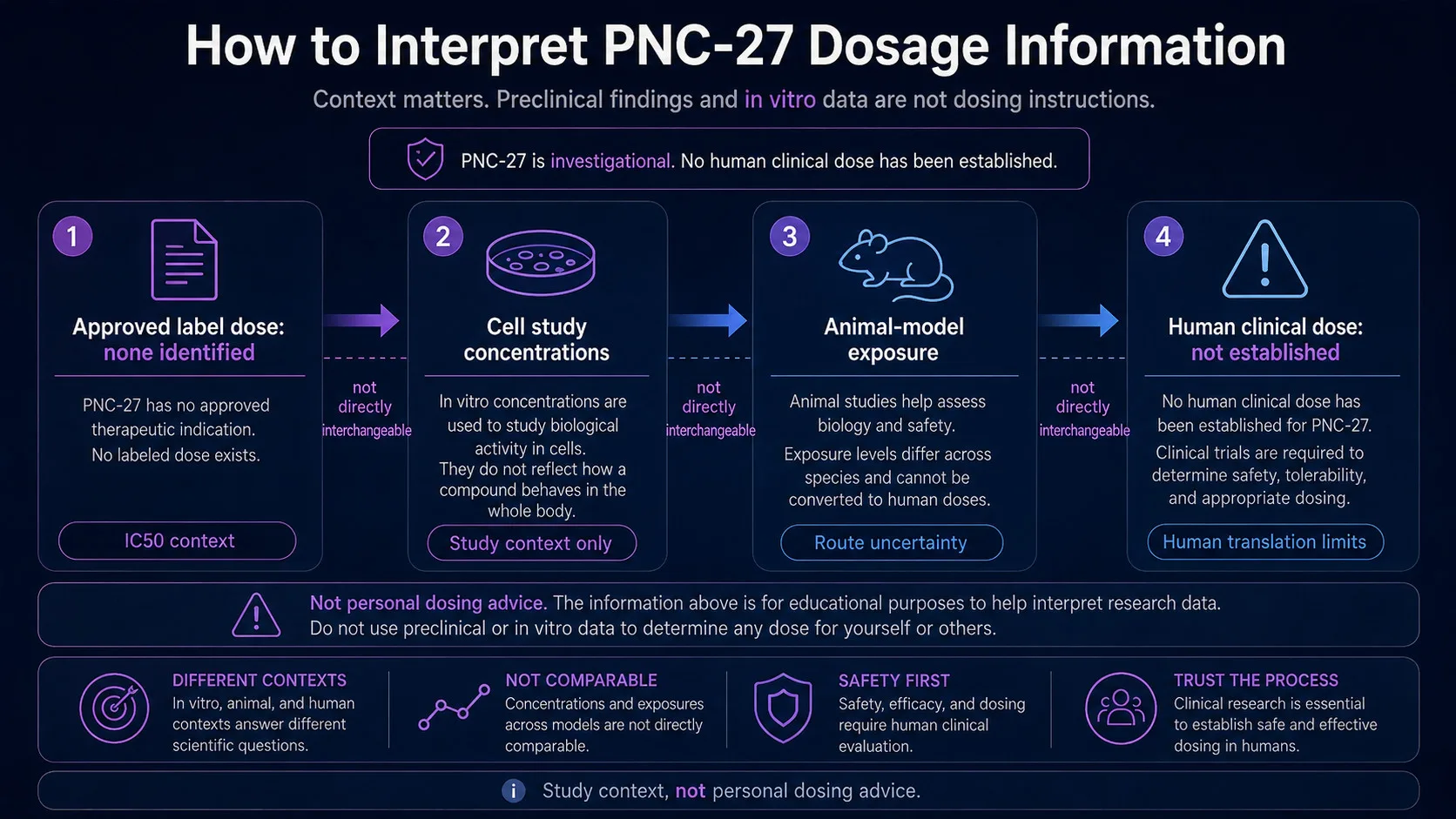
There is no FDA-approved PNC-27 dosage because PNC-27 is not listed as an approved drug with prescribing information in FDA public drug databases [14], [15]. Published preclinical studies may report cell-culture concentrations, IC50 values, or animal-model exposure, but those are study-context data and should not be interpreted as personal dosing advice [2], [3], [16].
| Dosage Context | What It Means | What It Does Not Mean |
|---|---|---|
| Approved label dose | No approved PNC-27 label dose is identified in FDA public drug databases [14], [15]. | No standard therapeutic protocol is established. |
| In vitro concentration | Cell studies may expose cancer cell lines to defined concentrations and measure viability or IC50-like endpoints [2], [3]. | Cell-culture concentrations are not human doses. |
| Animal-model exposure | Preclinical animal studies can test systemic or tumor-model effects under controlled conditions [2], [16]. | Animal dosing cannot be directly converted into safe human use. |
| Human clinical dose | No established PNC-27 human dosing program is identified in public trial and approval searches by name [14], [15], [16]. | There is no evidence-based personal dosing recommendation. |
No Approved Label Dose or Standard Therapeutic Protocol
No approved label means there is no regulator-reviewed dosing schedule, route, dose adjustment, contraindication list, adverse-reaction table, or drug-interaction section for PNC-27 [14], [15]. This is why phrases such as “PNC-27 protocol,” “best dose,” or “cycle” are not medically responsible outside a qualified research context [16], [17], [22].
Approved labeling matters because it reflects a specific product, indication, formulation, studied population, route, and safety dataset. PNC-27 does not currently have that approved-drug framework in FDA databases [14], [15].
Study Concentrations, IC50 Reporting, and Non-Personalized Interpretation
In cell biology, IC50 is a research metric that estimates the concentration associated with a half-maximal effect in an assay. PNC-27 cell line studies may use different concentrations of PNC-27 to assess cytotoxic effect, but those values depend on assay design, cell line biology, exposure time, peptide stability, and measurement method [2], [3].
Study doses should not be interpreted as personal dosing advice. Translating from cells to animals to humans requires pharmacokinetics, toxicology, dose-escalation studies, route-specific safety assessment, and regulatory oversight [16], [17], [22].
Administration Routes Discussed in PNC-27 Literature
PNC-27 administration routes should be discussed only as research context. The literature includes cell-culture exposure and preclinical animal-model administration, while no approved human route is established in FDA labeling [2], [14], [15], [16].
Route matters because pharmacokinetics, bioavailability, immune response, tissue exposure, and toxicity can differ depending on how a peptide is administered. For PNC-27, these questions remain unresolved in an approved clinical context [14], [15], [16].
Routes Used in Laboratory and Animal Research
In vitro studies expose cancer cells directly to the peptide in controlled culture conditions, which is not a patient administration route [2], [3]. Animal studies may use research-specific administration methods, but those methods cannot be translated into self-administration instructions or human dosing protocols [16], [22].
No step-by-step injection, mixing, or reconstitution information is appropriate for an unapproved investigational peptide. Any future human administration would need to occur under qualified clinical oversight with ethics review, product quality controls, safety monitoring, and regulatory compliance [16], [17], [22].
Why Administration Details Are Not Personal Use Instructions
Administration details in a paper are part of the experimental method, not a recommendation for personal use. A method section describes how a study was conducted; it does not establish that the same route, product, dose, or schedule is safe or effective for people [16], [22].
This point is especially important for peptides purchased outside regulated drug channels. FDA materials warn that unapproved drugs and compounded products may lack FDA review for safety, effectiveness, quality, and labeling, which can create additional risks [17], [18].
Is PNC-27 FDA-Approved? Regulatory and Legal Status
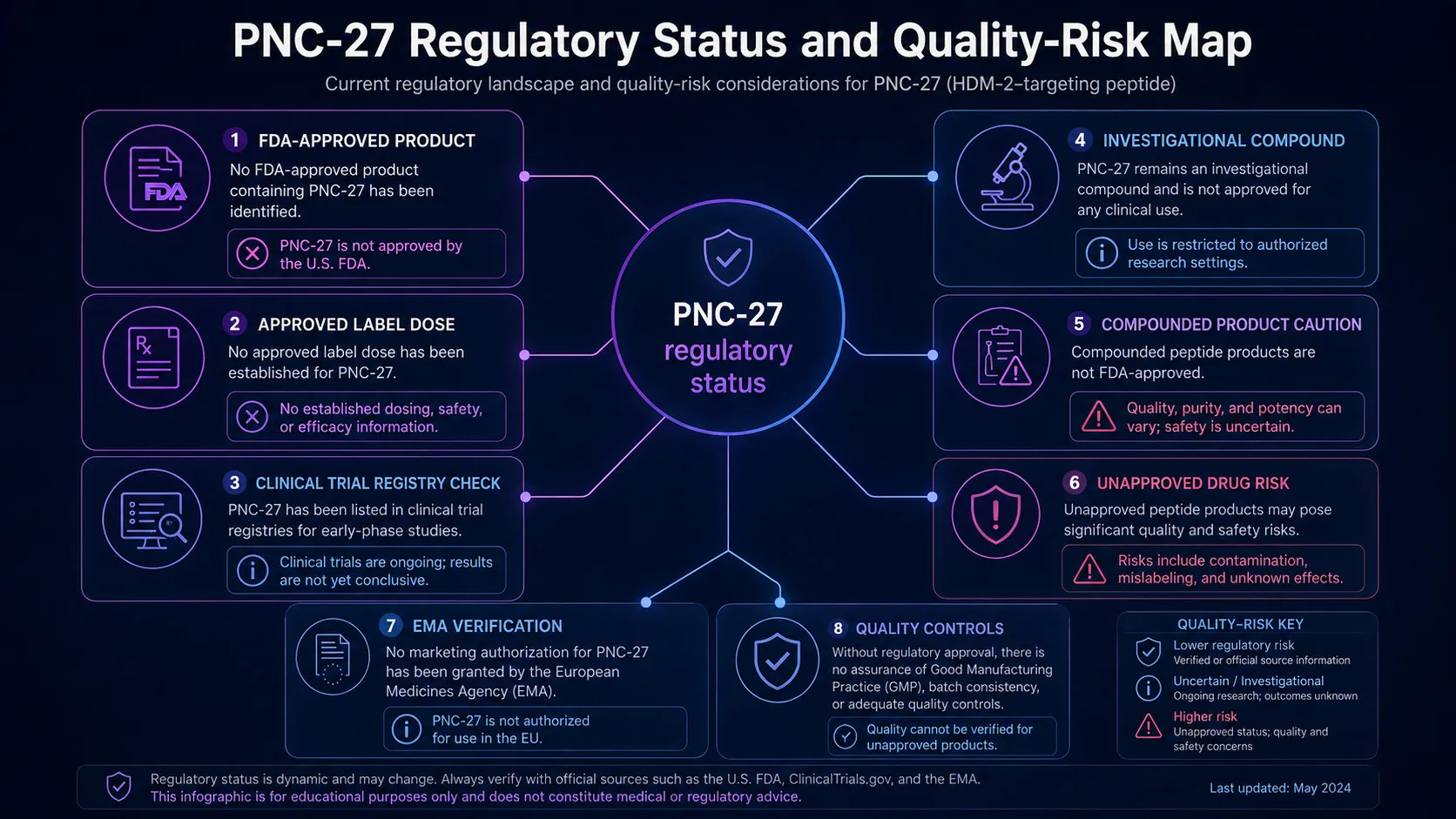
PNC-27 is not identified as an FDA-approved drug product in public FDA approval databases when searched by name, and no approved PNC-27 prescribing information is available through those databases [14], [15]. A direct ClinicalTrials.gov search by the term PNC-27 also does not identify a registered clinical study record at article preparation [16].
Regulatory status can vary by country and should be verified through official national or regional sources. EMA’s medicines database is an example of a regional regulator resource that can be checked for authorized medicines in the European Union 19.
Investigational Status and Absence of Approved Indications
The NCI Drug Dictionary entry helps identify PNC-27 as a research-stage compound with potential antineoplastic activity, but a dictionary entry is not the same as drug approval [1], [14], [15]. FDA approval requires evidence for a specific product, indication, manufacturing process, labeling, safety profile, and benefit-risk assessment [14], [18].
The absence of an approved indication means PNC-27 should not be described as a proven cancer therapy. It is more accurate to describe it as an investigational p53-derived anti-cancer peptide studied in preclinical cancer models [1], [2], [3], [16].
Risks of Unapproved, Compounded, or Research Peptides for Human Use
Unapproved or compounded peptide products may raise risks related to identity, purity, dose accuracy, sterility, contaminants, storage, and labeling. FDA explains that compounded drugs are not FDA-approved and are not reviewed by FDA for safety, effectiveness, or quality before they are marketed [17].
Research peptides sold online should not be assumed to be equivalent to approved medicines or to materials used in controlled studies. Regulatory status matters because product quality, legal status, and clinical oversight can directly affect safety [17], [18].
How Does PNC-27 Compare With Related Anti-Cancer Approaches?
PNC-27 differs from many related anti-cancer approaches because its proposed mechanism centers on HDM-2-associated cancer cell membrane disruption and pore formation [1], [3]. Conventional chemotherapy and immunotherapy are broader treatment categories with established clinical roles, risks, and regulatory oversight for specific indications [20], [21].
It also differs from intracellular MDM2 antagonist strategies. Small-molecule MDM2 inhibitors were designed to disrupt p53-MDM2 interactions and activate p53 pathways in selected contexts, whereas PNC-27 is discussed as a membrane-active peptide that may induce tumor cell necrosis [1], [11], [12].
PNC-27 Versus PNC-28, Chemotherapy, and Cancer Immunotherapy
PNC-28 is another p53-derived investigational peptide described by the NCI Drug Dictionary, but it is a distinct compound and should not be treated as interchangeable with PNC-27 4. Related names can confuse readers, so comparison should focus on mechanism, evidence level, approved status, and safety data rather than claims about which peptide is “best” [1], [4], [14], [16].
Compared with chemotherapy or immunotherapy, PNC-27 has a much weaker clinical evidence base. Chemotherapy and immunotherapy include approved treatments for specific cancers, while PNC-27 remains investigational and preclinical in the available public evidence landscape [14], [15], [20], [21].
Key Takeaways and Questions to Discuss With a Clinician
The safest way to interpret PNC-27 is through evidence quality, regulatory status, safety data, and clinician-guided decision-making. The strongest available support is mechanistic and preclinical, while human efficacy, human dosing, side effects, contraindications, interactions, and long-term safety remain unresolved [1], [2], [3], [14], [16].
A practical clinician discussion checklist may include:
- What is the confirmed diagnosis, stage, tumor biology, and standard-of-care treatment plan? [20], [21]
- Is there any legitimate clinical trial involving PNC-27 or a related agent? [16], [22]
- What evidence level supports the claim: approved label, clinical trial, early human evidence, preclinical study, or anecdote? [14], [16], [22]
- Could an investigational peptide interfere with chemotherapy, immunotherapy, radiation, surgery, supportive care, labs, or trial eligibility? [16], [20], [21]
- What is known about product quality, sterility, identity, and regulatory oversight? [17], [18]
- Are safer, approved, or trial-based alternatives available for the specific cancer type? [14], [20], [21]
What Remains Unknown About PNC-27 Safety, Efficacy, and Appropriate Use
Major unknowns include whether PNC-27 reliably reaches tumor tissue in humans, whether HDM-2 in cancer cell membranes is a consistent target across patient tumors, what dose and route would be tolerable, whether normal cells or organs could be harmed, and whether tumor cell necrosis in models translates into meaningful clinical benefit [1], [2], [3], [16]. Long-term safety, pregnancy and breastfeeding risk, drug interactions, immunologic effects, pharmacokinetics, bioavailability, metabolism, and adverse-event rates are also not established in approved labeling [14], [15], [16].
The most responsible conclusion is cautious: PNC-27 peptide is a biologically interesting investigational anti-cancer peptide, but current public evidence does not support treating it as an approved or proven cancer therapy. Readers considering peptide-related medical decisions should discuss evidence, risks, alternatives, clinical trials, and regulatory status with a qualified healthcare professional.
REFERENCES
- National Cancer Institute. PNC-27. NCI Drug Dictionary. Accessed 2026.
- National Center for Biotechnology Information. PNC-27 peptide indexed literature search. PubMed database. Accessed 2026.
- National Center for Biotechnology Information. PNC-27 HDM-2 pore formation indexed literature search. PubMed database. Accessed 2026.
- National Cancer Institute. PNC-28. NCI Drug Dictionary. Accessed 2026.
- UniProt Consortium. Cellular tumor antigen p53 — TP53, UniProtKB P04637. UniProtKB. Accessed 2026.
- UniProt Consortium. E3 ubiquitin-protein ligase Mdm2 — MDM2, UniProtKB Q00987. UniProtKB. Accessed 2026.
- Momand J, Zambetti GP, Olson DC, George D, Levine AJ. The mdm-2 oncogene product forms a complex with the p53 protein and inhibits p53-mediated transactivation. Cell. 1992.
- Kussie PH, Gorina S, Marechal V, et al. Structure of the MDM2 oncoprotein bound to the p53 tumor suppressor transactivation domain. Science. 1996.
- Haupt Y, Maya R, Kazaz A, Oren M. Mdm2 promotes the rapid degradation of p53. Nature. 1997.
- Kubbutat MHG, Jones SN, Vousden KH. Regulation of p53 stability by Mdm2. Nature. 1997.
- Wade M, Li YC, Wahl GM. MDM2, MDMX and p53 in oncogenesis and cancer therapy. Nature Reviews Cancer. 2013.
- Vassilev LT, Vu BT, Graves B, et al. In vivo activation of the p53 pathway by small-molecule antagonists of MDM2. Science. 2004.
- Gaspar D, Veiga AS, Castanho MARB. From antimicrobial to anticancer peptides: a review. Frontiers in Microbiology. 2013.
- U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs. FDA database. Accessed 2026.
- U.S. Food and Drug Administration. Approved Drug Products with Therapeutic Equivalence Evaluations — Orange Book. FDA database. Accessed 2026.
- U.S. National Library of Medicine. ClinicalTrials.gov search: PNC-27. ClinicalTrials.gov. Accessed 2026.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. FDA. Accessed 2026.
- U.S. Food and Drug Administration. Unapproved Drugs. FDA. Accessed 2026.
- European Medicines Agency. Medicines database. EMA. Accessed 2026.
- National Cancer Institute. Chemotherapy to Treat Cancer. NCI. Accessed 2026.
- National Cancer Institute. Immunotherapy to Treat Cancer. NCI. Accessed 2026.
- U.S. National Library of Medicine. Learn About Clinical Studies. ClinicalTrials.gov. Accessed 2026.
FAQs
What is PNC-27 peptide?
PNC-27 peptide is an investigational p53-derived peptide studied for possible membrane-targeted anti-cancer activity, especially through interaction with HDM-2 on cancer cell membranes [1]. It is discussed in peptide research because its design combines a p53-related binding concept with a membrane residency component [1]. Public FDA databases do not identify an approved PNC-27 drug product or approved indication, so clinical use is not established [14], [15].
What are the potential benefits of PNC-27 peptide?
Potential benefits of PNC-27 peptide are mainly preclinical and should not be read as proven patient outcomes. Laboratory work has explored whether PNC-27 can be cytotoxic to cancer cells, produce tumor cell death, and show anti-tumor activity through membrane disruption [1], [2], [3]. What remains unproven is clinical benefit, such as tumor response, longer survival outcomes, or safer treatment compared with established oncology care [16].
How does PNC-27 peptide interact with HDM-2?
PNC-27 peptide is proposed to interact with the HDM-2 protein at or near the cancer cell membrane [1], [3]. The concept comes from a p53-related binding domain and differs from many intracellular MDM2-blocking strategies. In preclinical models, researchers have discussed pore formation, cell lysis, and the idea that PNC-27 induces necrosis in tumor cells [1], [3]. This mechanism remains a research hypothesis, not proof of human efficacy.
What types of cancer has PNC-27 been studied in, including breast cancer?
PNC-27 has been discussed in preclinical cancer cell line research, including contexts involving breast cancer, pancreatic cancer, leukemia-related cells, and other tumor models [2], [3]. These studies can examine whether the peptide affects cancer cells under laboratory conditions. They do not prove that PNC-27 is effective for breast cancer, first-line therapy, or any cancer treatment in humans, because clinical tumor response and survival outcomes are not established [16].
Are there known side effects or serious safety concerns with PNC-27 peptide?
Known side effects of PNC-27 peptide are not well characterized in humans because there is no approved prescribing information or label-based adverse-reaction table for an approved PNC-27 product [14], [15]. The lack of a label also means there are no product-specific black box warnings, but that should not be interpreted as evidence of safety. Serious side effects, allergic reactions, organ risks, and drug combination risks remain uncertain without adequate human studies.
What dosage information and regulatory status exist for PNC-27 peptide?
Dosage information for PNC-27 peptide does not include an approved label dose, because public FDA databases do not identify an approved PNC-27 drug product [14], [15]. Published research may describe cell-culture concentrations or animal-model exposure, but those data are not personal dosing advice [2], [3]. Legal status can vary by jurisdiction, and unapproved or compounded products raise quality, sterility, identity, and regulatory concerns [17], [18], [19].
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Arnold J. Levine
Author profile: Institute for Advanced Study Profile
Arnold J. Levine’s published work is central to the broader p53 and HDM-2/MDM2 context needed to interpret PNC-27 peptide research. His coauthored studies helped define how MDM2 interacts with p53 and how the p53 transactivation domain can bind the MDM2 oncoprotein. This background is relevant to the mechanism-of-action discussion in this article, especially the distinction between p53-derived peptide concepts, MDM2-binding biology, and the limits of translating preclinical mechanism findings into clinical evidence.
Selected publications:
- The mdm-2 oncogene product forms a complex with the p53 protein and inhibits p53-mediated transactivation — Cell, 1992. PMID: 1535557
- Structure of the MDM2 oncoprotein bound to the p53 tumor suppressor transactivation domain — Science, 1996. PMID: 8875929
Karen H. Vousden
Author profile: PubMed Author Search
Karen H. Vousden’s publications are relevant to the p53 pathway, MDM2-mediated regulation of p53 stability, and evidence-based interpretation of p53-centered cancer biology. Her work helps frame why p53-derived and MDM2-related strategies are scientifically important while also underscoring that mechanistic relevance is not the same as established clinical use. This context supports the article’s cautious treatment of PNC-27 as an investigational peptide whose preclinical research should be separated from proven therapeutic outcomes.
Selected publications:
- Regulation of p53 stability by Mdm2 — Nature, 1997. PMID: 9153396
- Blinded by the Light: The Growing Complexity of p53 — Cell, 2009. PMID: 19766790